Patellofemoral Pain Syndrome is a common cause of discomfort at the front of the knee. It often results from poor movement mechanics, muscular imbalance, or repetitive stress on the joint. While frequently associated with active individuals, it can affect anyone with increased knee demand. This article outlines typical causes, effective management strategies, and the role of bracing and rehabilitation exercises in restoring knee function.

Patellofemoral Pain Syndrome (PFPS), commonly referred to as “runner’s knee,” is one of the most frequent causes of anterior knee pain, especially among physically active individuals. It occurs when the patella (kneecap) does not track properly along the trochlear groove of the femur during movement, leading to irritation of the surrounding soft tissues or the articular cartilage beneath the patella. PFPS is not typically associated with structural damage but rather functional imbalances, making it a diagnosis of exclusion. It is most prevalent in adolescents, young adults, and athletes, particularly females, and is strongly linked to overuse and biomechanical dysfunction of the lower extremity.
Symptoms of PFPS often develop gradually and may vary depending on activity level. Common symptoms include:
PFPS is considered a multifactorial condition resulting from poor patellar tracking, muscular imbalance, and excessive joint loading. Common causes include:
Effective treatment for PFPS focuses on reducing pain, correcting biomechanical imbalances, and restoring functional movement. Management strategies include:

Bracing can be an effective adjunctive strategy in the conservative management of patellofemoral pain syndrome (PFPS), particularly when integrated with exercise therapy and load management. Patellar tracking braces are designed to optimize joint alignment, reduce pain, and support functional recovery. The therapeutic effects of bracing include:
Rehabilitation exercises for PFPS aim to strengthen the muscles that stabilize the patella and improve overall lower limb alignment. Common exercises include:

Straight leg raises and terminal knee extensions help activate the quadriceps, particularly the VMO.
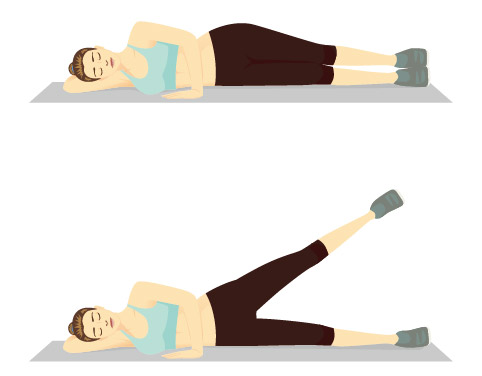
Side-lying leg lifts, clamshells, and band walks target the gluteus medius and external rotators to improve dynamic knee alignment.
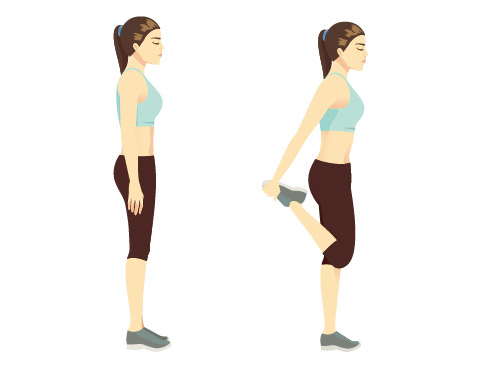
Regular stretching of the IT band, hamstrings, hip flexors, and calves can reduce excessive tension on the knee joint.
Controlled step-down exercises help train eccentric strength and proper knee alignment during functional movement.
These help restore quadriceps endurance while minimizing patellofemoral joint load when performed within a pain-free range.
Single-leg stance and balance board exercises improve neuromuscular control and prevent future dysfunction.
Walli, O., McCay, M., & Tiu, T. K. (2023, March 14). Patellofemoral syndrome: A review of diagnosis and treatment. Current Physical Medicine and Rehabilitation Reports, 11(2), 139–143.
Madou, K. H. (2023, February 6). Patellofemoral (anterior knee) pain syndrome: Symptoms, causes and guideline-based treatment options. MOJ Sports Medicine, 6(1), 23–26.
Wiguna, I. G. L. N. A., & Setiawan, C. R. (2022, May). Patellofemoral pain syndrome: Literature review. International Journal of Scientific and Research Publications, 12(5), 21. Phillips, R., Choo, S., & Nuelle, C. (2022). Bracing for the patellofemoral joint. The Journal of Knee Surgery.
Kölle, T., Alt, W., & Wagner, D. (2020). Immediate effects of an elastic patellar brace on pain, neuromuscular activity and knee kinematics in subjects with patellofemoral pain. Archives of Orthopaedic and Trauma Surgery, 140, 905-912.
Sisk, D., & Fredericson, M. (2020). Taping, Bracing, and Injection Treatment for Patellofemoral Pain and Patellar Tendinopathy. Current Reviews in Musculoskeletal Medicine, 13, 537-544.
Palumbo, P. (1981). Dynamic patellar brace: A new orthosis in the management of patellofemoral disorders. The American Journal of Sports Medicine, 9, 45 - 49.
Sker, F., Anbarian, M., Yazdani, A., Hesari, P., & Babaei-Ghazani, A. (2017). Patellar bracing affects sEMG activity of leg and thigh muscles during stance phase in patellofemoral pain syndrome.. Gait & posture, 58, 7-12.
Petersen, W., Ellermann, A., Rembitzki, I., Scheffler, S., Herbort, M., Brüggemann, G., Best, R., Zantop, T., & Liebau, C. (2016). Evaluating the potential synergistic benefit of a realignment brace on patients receiving exercise therapy for patellofemoral pain syndrome: a randomized clinical trial. Archives of Orthopaedic and Trauma Surgery, 136, 975 - 982.
Taghipourdarzinaghibi, M., Hosseinzadeh, S., & Eslami, M. (2018). Comparisons of bracing and patella taping on knee three-dimensional kinematics of women with patellofemoral pain syndrome in stance phase of running. Annals of Physical and Rehabilitation Medicine.
Lun, V., Wiley, J., Meeuwisse, W., & Yanagawa, T. (2005). Effectiveness of Patellar Bracing for Treatment of Patellofemoral Pain Syndrome. Clinical Journal of Sport Medicine, 15, 235-240.
Arazpour, M., Notarki, T., Salimi, A., Bani, M., Nabavi, H., & Hutchins, S. (2013). The effect of patellofemoral bracing on walking in individuals with patellofemoral pain syndrome. Prosthetics and Orthotics International, 37, 465 - 470.
Alshaharani, M., Lohman, E., Bahjri, K., Harp, T., Alameri, M., Jaber, H., & Daher, N. (2020). Comparison of Protonics™ Knee Brace to Sport Cord on Knee Pain and Function in Patients With Patellofemoral Pain Syndrome: A Randomized Controlled Trial.. Journal of sport rehabilitation, 1-30.
Copy Link